This web page was produced as an assignment for Genetics 677, an undergraduate course at UW-Madison.
Project Goal
|
About Site Author
|
Introduction
Rett Syndrome is a neurodevelopmental disorder primarily affecting females. 1 in 10,000 females are born with Rett Syndrome. It occurs in all racial and ethnic groups throughout the world. Rett syndrome is not inherited and is caused by random mutations which usually occur during spermatogenesis. |

Figure 1: Rett syndrome primarily affects females. |
Rett Syndrome has four stages.
Stage 1: Early Onset
This stage begins between 6 and 18 months and is often overlooked. Symptoms are characterized as a subtle lag in development. Infants may show less eye contact and interest in toys. They may also have delayed gross motor skills.
Stage 2: Rapid Destructive
This stage begins between 1 and 4 years and persists for multiple weeks or months, progressing either rapidly or gradually. Characteristic hand movements, such as wringing, clapping, or tapping emerge. Some children also move their hands to their mouths repeatedly or clasp them behind their backs. Breathing may also be irregular in the form of both apnea and hyperventilation. Symptoms may mimic autism in some children, as they have reduced social interaction and communication. Gross motor skills and head growth are also delayed.
Stage 3: Plateau
This stage occurs between 2 and 10 years and may last for several years or the rest of their lives. Problems with motor skills and seizures are prevalent during this stage, though children may become have improved behavior and less irritability. Children in this stage may also become more alert and attentive as well as showing more interest in her surroundings.
Stage 4: Late Motor Deterioration
This stage may last for several years or the rest of their lives. The muscles become weak, rigid, or spastic. This may make it difficult or impossible for them to walk. Children may also have scoliosis. Communication and cognition usually remain constant and gaze fixation may improve. (1)
MECP2

Figure 2: Locaiton of MECP2 on the X Chromosome and the Methyl-CpG binding domain of MECP2 (3).
The MECP2 gene is found on the q arm of the X chromosome on position 28. It is comprised of 4 exons and is 76,189 bases long. (3) During X inactivation, the normal MECP2 copy is randomly inactivated in some cells, causing a range of symptoms. (1)
Rett Syndrome is caused by random mutations in the MECP2 gene which change the structure or lower the amount of MeCP2 protein in the cell. Thus, the genes that MeCP2 normally silences remain expressed and unnecessary proteins are created. (3) MECP2 is expressed in many tissues, but is most highly expressed in mature neurons. This is also where the lack of MECP2 has the highest impact. (5)
The Methyl CpG binding protein 2 (MeCP2) is needed for normal brain development. Studies suggest that MeCP2 is essential for forming synapses between nerve cells by silencing genes that encode proteins involved in synaptic formation when they are not needed. Specifically, MeCP2 represses transcription at methylated CpG sites by recruiting the mSin3a corepressor which contains histone deacetylaces that repress the transcription of genes with CpG sites (4). MeCP2 may also be involved with alternative splicing in mRNA which encodes proteins needed for accurate communication between nerve cells. (3)
Domain Structure and Proposed Function
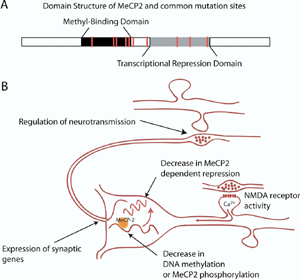
Studies have shown that a loss of MECP2 function causes changes in spontaneous synaptic activity as well as short and long term synaptic plasticity. MECP2 represses the transcription of several genes, such as Sin3A, and HDAC1, HDAC2. These proteins form a complex that are also involved in transcriptional repression and inhibit the production of certain synaptic proteins. Activity dependent MECP2 phosphorylation inactivates the protein and allows MECP2's target genes to remain unmethylated. This allows MECP2 to regulate when certain genes are expressed. This suggests that MECP2 may play a role in a homeostatic mechanism regulating neurotransmitter output. (5)
Figure 3: A - Domain sturcture of MECP2 with sights of mutations associated with Rett Syndrome (red lines). B - The relationship between MECP2 protein and synaptic activity. Removial of MECP2 my lead to an increase in transcription of genes that regulate neurotransmission. (5)
"Live With Rett Syndrome" features the reactions of families with a daughter with Rett Syndrome to research that found that Rett Syndrome symptoms could be reversed in mice. To learn more about this study, go to the literature page.
Recent Site Visitors
References
1. National Institute of Neurological Disorders and Stroke. (2008, June 6) Rett Syndrome Fact Sheet. Retrieved February 2, 2009, from http://www.ninds.nih.gov/disorders/rett/detail_rett.htm.
2. (Figure 1) Families.com. (2006, June 10) Rett Syndrome: A Brief Overview. Retrieved February 27, 2009, from http://special-needs.families.com/blog/rett-syndrome-a-brief-overview.
3. (Figure 2) Society for Neuroscience (2009) Brain Briefings - Rett Syndrome. Retrieved February 12, 2009 from http://www.sfn.org/skins/main/images/brainbriefings/bb_April2007_large.jpg.
4. Entrez Gene. (2009, January 12) MECP2 methyl CpG 2 binding protein (Rett Syndrome). Retrieved February 2, 2009 from http://www.ncbi.nlm.nih.gov/entrez/dispomim.cgi?id=300005.
5. (Figure 3) Monteggia, L.M., Kavalali, E.T. (2009) Rett syndrome and the impact of MeCP2 associated transcriptional mechanisms on neurotransmission. Biological Psychiatry 65 (3) 204-10
6. U.S. National Library of Medicine (2009, January 30) Genetics Home Reference: MECP2. Retrieved February 2, 2009, from http://ghr.nlm.nih.gov/gene=mecp2.
7. (Header Photograph) Adapted from: Naser, S. How Stuff Works. How Brain Mapping Works. Retrieved February 2, 2009, from http://health.howstuffworks.com/brain-mapping.htm.
Jessica Connor
[email protected]
Last Updated: 3/1/09

{kind=link}